Daniel Brison, MD, Pedram Ilbeigi, DO, and Hossein Sadeghi-Nejad, MD
A B S T R A C T
Introduction.We describe a 51-year-old man with a history of radiation therapy and large bowel diversion for rectal cancer who underwent an uneventful penile implant surgery for erectile dysfunction that was refractory to conservative therapy. The patient presented with acute left lower extremity swelling and pain a few days after surgery. Workup revealed compression of the pelvic veins by the prosthesis reservoir.
Aim.To highlight an avoidable, adverse event related to penile prosthesis reservoirs.
Methods.Retrospective review of a clinical case.
Results.The patient underwent repositioning of the reservoir followed by venous thrombectomy and Greenfield filter placement.
Conclusion.To the best of our knowledge, this is the first report of an early diagnosis and successful thrombectomy of the external iliac and common femoral vein thrombosis secondary to reservoir compression. Awareness of this possible adverse event and the management strategy are helpful to surgeons who perform penile prosthesis surgery. Brison D, Ilbeigi P, and Sadeghi-Nejad H. Reservoir repositioning and successful thrombectomy for deep venous thrombosis secondary to compression of pelvic veins by an inflatable penile prosthesis reservoir. J Sex Med 2007;4:1185–1187.
Key Words.Penile Prosthesis; Complications, Deep Venous Thrombosis
Introduction
Three-piece penile prostheses were introduced approximately 30 years ago and are now a widely used treatment modality for erectile dysfunction [1]. Superb mechanical reliability and resilience, as well as excellent patient and partner satisfaction levels, have contributed to the increasing number of cases performed in the United States [2,3].
Device infection, retained segments, mechanical failure, corporal crossover, corporal and urethral perforation, erosions, and reservoir herniation are among the reported complications in the literature [4–8]. There have only been two reported cases of reservoir complications leading to venous compromise and thrombus formation. To the best of our knowledge, this is the first report of an early diagnosis and successful thrombectomy of the external iliac and common femoral vein thrombosis secondary to reservoir compression.
Case Report
A 51-year-old man with a history of radiation therapy and large bowel diversion surgery for rectal cancer underwent uneventful penile implant surgery through a penoscrotal incision for organic erectile dysfunction. The patient had previously failed oral therapy with phosphodiesterase inhibitors. Intraurethral and intracavernous prostaglandin E1 treatments had been similarly unsuccessful.
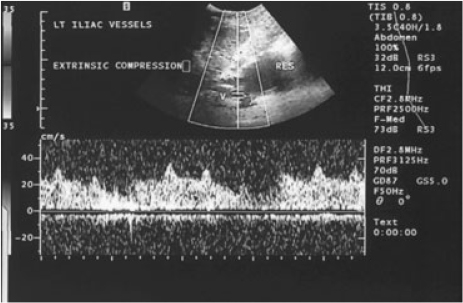
On postoperative day number four, he returned to the emergency room complaining of left lower extremity (LLE) swelling and pain. The physical examination revealed a healing scrotal incision, but was remarkable for LLE edema, erythema, and tenderness to palpation. Venous Doppler sonography revealed sluggish flow consistent with a prethrombotic state in the left distal external iliac and common femoral veins due to reservoir compression (Figure 1). The penile implant was fully inflated to decrease the reservoir size and decrease vascular compression.
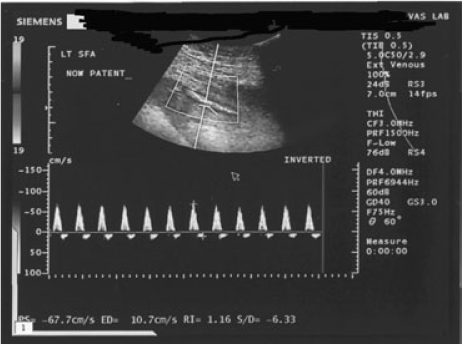
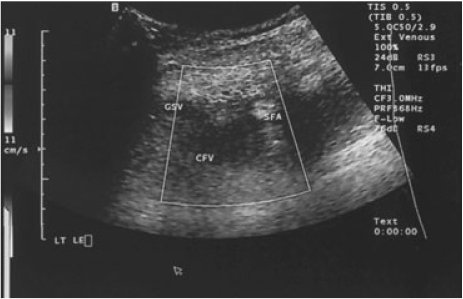
The patient was taken to the operating room for repositioning of the reservoir shortly after presentation. Through a small suprapubic exploratory incision, the reservoir was found to be compressing the pelvic veins (due to the severe scarring from the previous bowel/pelvic surgery) and was easily repositioned away from the vessels. The patient was later monitored in an intensive care unit while placed in a Trendelenburg position on a heparin drip. Despite clinical improvement in the immediate postoperative period, LLE swelling and pain recurred 8 hours later. A repeat Doppler sonography demonstrated thrombosis of the left distal external iliac through superficial femoral veins with no evidence of residual compression by the repositioned reservoir. There was no color Doppler flow and intraluminal thrombus material was visible (Figures 2 and 3). The vascular surgery service was consulted and a decision was made to proceed with venous thrombectomy and Greenfield filter placement. The patient’s recovery was uneventful. He was discharged home several days after admission with complete resolution of his LLE swelling and normal function of his penile prosthesis.
Discussion
Proper placement of a reservoir in the retropubic space can be challenging in patients with prior pelvic surgery or a history of radiation therapy. Blunt and/or sharp dissection for the creation of a paravesical, retropubic space of adequate size that will allow expansion of the reservoir without lateral migration is critical to the normal operation of this component. In this case, the combination of a diverting colostomy and radiation therapy contributed to the formation of numerous thick adhesions. The initial reservoir placement was not difficult and a separate suprapubic incision for reservoir placement was not deemed necessary. In retrospect, the latter may have helped to avert vascular compression. However, we believe reservoir inflation against pelvic adhesions caused lateral displacement and compression of the femoral vessels. Therefore, awareness of this potential complication and a more focused attempt at reservoir placement away from the lateral vessels through the original penoscrotal incision may have been equally successful.
The patients’ awareness of this unusual adverse event and thus early presentation as well as prompt recognition of deep venous thrombosis (DVT) secondary to reservoir compression are of great importance in successful management of this complication. Early diagnosis will allow proper reservoir repositioning as well as a thrombectomy in due time to decrease the risk of further complications and the necessity of lifelong anticoagulation therapy. To the best of our knowledge, this is the first report of an early diagnosis and successful thrombectomy of the external iliac and common femoral vein thrombosis secondary to reservoir compression.
Reservoir complications are relatively uncommon and include herniation with inguinal scrotal migration or, rarely, erosion into adjacent viscera [4–8]. Although a previous case report noted significant vein narrowing and compression masquerading as a DVT, true DVT secondary to reservoir compression has been reported only once in the literature [8,9]. In the latter report, the patient had previously undergone a radical retropubic prostatectomy and presented with acute DVT 3 days after surgery. Thrombectomy had not been performed due to the existing DVT and mild edema of the lower extremities persisted after reservoir revision. The fortunate early presentation in our case led to immediate recognition of the clinical scenario and successful thrombectomy by the vascular surgeons. Occasionally, surgeons will perform a second lateral incision for reservoir placement in patients with a history of radical retropubic prostatectomy or radical cystectomy. More importantly, it is critical to have a low threshold for rechecking proper reservoir placement away from the lateral vessels in all cases with extensive abdominal or pelvic surgery or a history of pelvic irradiation.
Conclusions
Reservoir compression of the pelvic vessels is a rare, but serious adverse event that can be avoided by making a conscious effort for a more precise and controlled placement of the reservoir away from the lateral pelvic vessels. This is especially important in cases with extensive abdominal or pelvic surgery or a history of pelvic irradiation. With early recognition, DVT due to reservoir compression may be successfully managed by reservoir repositioning and thrombectomy when appropriate.
Corresponding Author:Hossein Sadeghi-Nejad, MD, UMDNJ New Jersey Medical School, Department of Surgery, Division of Urology, 185 South Orange Ave, MSB G 536, Newark, NJ 07103-2714, USA. Tel: (973) 972-4488; Fax: (973) 395-7197
Conflict of Interest:None.
References
- Scott FB, Bradley WE, Timm GW. Management of erectile impotence. Use of implantable inflatable prosthesis. Urology 1973;2:80–2.
- Brinkman MJ, Henry GD, Wilson SK, Delk JR 2nd, Denny GA, Young M, Cleves MA. A survey of patients with inflatable penile prostheses for satisfaction. J Urol 2005;174:253–7.
- Carson CC, Mulcahy JJ, Govier FE. Efficacy, safety and patient satisfaction outcomes of the AMS 700CX inflatable penile prosthesis: Results of a long-term multicenter study. AMS 700CX Study Group. J Urol 2000;164:376–80.
- Ilbeigi P, Sadeghi-Nejad H, Kim M. Retained reartip extenders in redo penile prosthesis surgery: A case for heightened suspicion and thorough physical examination. J Sex Med 2005;2:149–50.
- Munoz JJ, Ellsworth PI. The retained penile prosthesis reservoir: A risk. Urology 2000;55:949.
- Nelson RP Jr. Small bowel obstruction secondary to migration of an inflatable penile prosthesis reservoir: Recognition and prevention. J Urol 1988;139: 1053–4.
- Sadeghi-Nejad H, Sharma A, Irwin RJ, Wilson SK, Delk JR. Reservoir herniation as a complication of three-piece penile prosthesis insertion. Urology 2001;57:142–5.
- Singh I, Godec CJ. Asynchronous erosion of inflatable penile prosthesis into small and large bowel. J Urol 1992;147:709–10.
- da Justa DG, Bianco FJ Jr, Ogle A, Dhabuwala CB. Deep venous thrombosis due to compression of external iliac vein by the penile prosthesis reservoir. Urology 2003;61:462.
- Flanagan MJ, Krisch EB, Gerber WL. Complication of a penile prosthesis reservoir: Venous compression masquerading as a deep venous thrombosis. J Urol 1991;146:847–8.